March 2026
NewsletterSummary:
-
-
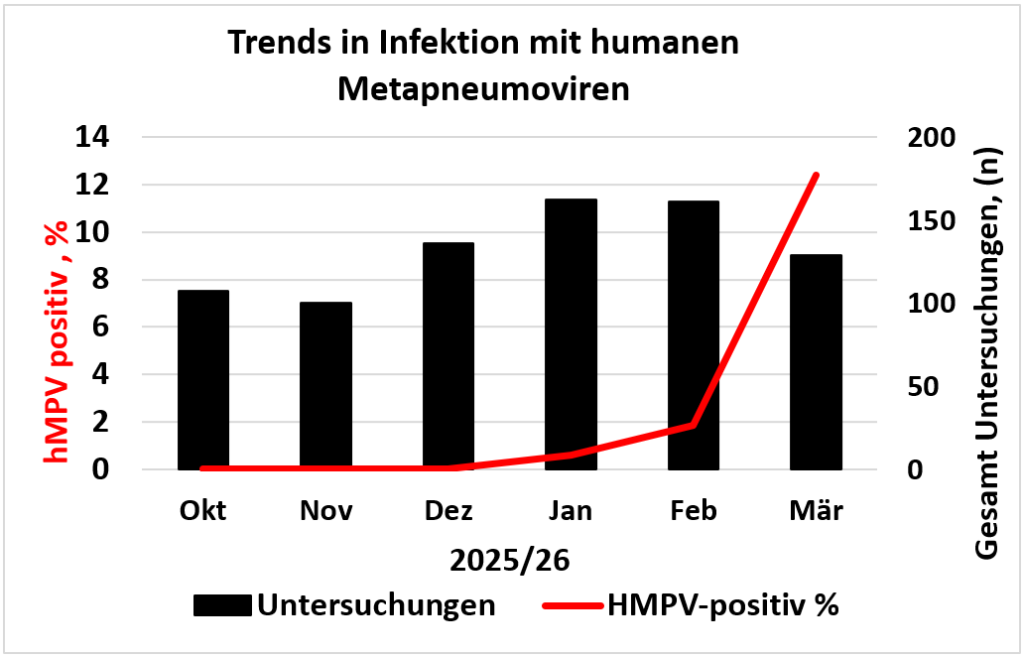
- hMPV positivity rates rose from 0.6% in January to over 12% in March 2026 — a pattern typical of temperate climates in late winter and spring.
- The respiratory multiplex PCR panel covering hMPV is used at the institute exclusively for inpatients and emergency department patients, as outpatient reimbursement is not available.
- Closely related to RSV, hMPV is the third most common viral cause of severe respiratory infections requiring hospitalisation, with infants and immunocompromised individuals at greatest risk.
- Transmission occurs via droplets, close contact, and surfaces; viral shedding typically lasts 5–10 days, but may extend well beyond two weeks in vulnerable groups.
- No specific antiviral treatment or licensed vaccine exists; prevention relies on standard hygiene measures.
-
Epidemiology of Human Metapneumovirus (hMPV) Infections
While RSV case numbers have declined over the past two weeks, a marked increase in human metapneumovirus (hMPV) infections is currently being observed. Although no hMPV was detected among a total of 340 respiratory multiplex PCRs performed within our cohort between October and December 2025, a successive rise in positivity rates has been recorded since the start of the year: from 0.6% in January to 1.8% in February and exceeding 12% in March (see figure). In temperate climates, hMPV typically peaks from late winter into spring — often immediately following the RSV peak.
The respiratory multiplex PCR panel, which also detects hMPV, is used at our institute exclusively for inpatient and emergency department patients, as reimbursement is currently not available for outpatient settings.
Since the majority of hMPV infections follow a mild course and remain confined to the upper respiratory tract — and therefore do not necessitate a hospital visit — it can be assumed that the prevalence in the general population and in outpatient settings is considerably higher.
hMPV is structurally and taxonomically closely related to RSV and causes similar, though generally somewhat milder, clinical presentations. Nevertheless, hMPV ranks — after RSV and influenza — among the most common viral causes of severe respiratory infections requiring hospitalisation or emergency admission. Primary infections, which can occasionally be severe, occur predominantly in early childhood.
Transmission takes place primarily via respiratory droplets, close contact, and contaminated surfaces. Viral shedding typically lasts 5–10 days, but can be considerably longer in infants and immunocompromised individuals — in some cases exceeding two weeks.
The infection is self-limiting and there is no specific antiviral therapy. As there is also no licensed vaccine, prevention relies on standard hygiene measures. Several experimental live-attenuated and subunit vaccines are in preclinical or early clinical development — individually or in combination with RSV or human parainfluenza viruses (https://clinicaltrials.gov/study/NCT03392389; Miller RJ 2023; Yu D 2025). A regulatory approval candidate is not currently in sight.

Priv.-Doz. Dr.med. Wegene Borena, PhD
wegene.borena@i-med.ac.at
+43 512 9003 71710